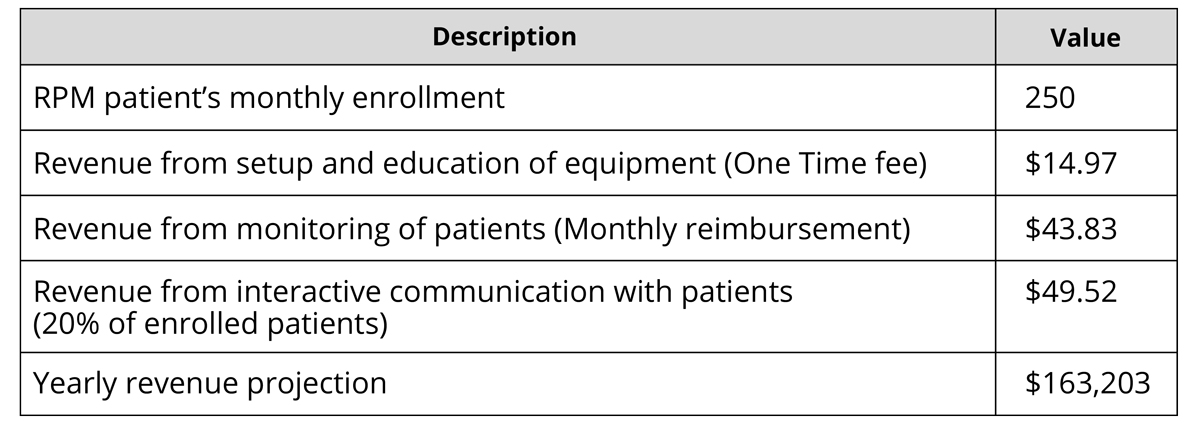
CMS announced in the 2019 Medicare Physician Fee Schedule Final Rule that it would reimburse three new RPM codes approved by the CPT Editorial Panel in September 2018, effective January 1, 2019:
CPT 99453: Remote monitoring of physiologic parameter(s) (e.g., weight, blood pressure, pulse oximetry, respiratory flow rate), initial; set-up and patient education on use of equipment.
CPT 99454: Remote monitoring of physiologic parameter(s) (e.g., weight, blood pressure, pulse oximetry, respiratory flow rate), initial; each 30 days.
CPT 99457: Remote physiologic monitoring treatment management services, 20 minutes or more of clinical staff/physician/other qualified health care professional time in a calendar month requiring interactive communication with the patient/caregiver during the month.
The OMS C3™ platform supports Remote Physiological Monitoring (RPM) of patients by offering a comprehensive Blue Tooth Enabled devices (BP Monitor, Weight Scale etc.) solution. This service offering provides tremendous power to the practice to be proactive in the management of patients with chronic diseases like Hypertension, Heart Failure and Atrial Fibrillation.