
Most cardiologists didn’t choose their EHR. It was chosen for them — usually by a hospital system or group purchasing decision that prioritized enterprise coverage over specialty fit. The result is familiar to anyone who has finished clinic and then spent the evening catching up on notes: a system designed for every specialty ends up optimized for none.
Cardiology is arguably the specialty where this mismatch costs the most. Few fields generate as much structured data — echos, caths, nuclear studies, ECGs, device interrogations, lipid panels, remote monitoring feeds — and few depend as heavily on connecting that data across time to make a decision in the exam room.
Where general EHRs fall short for cardiology
1. Diagnostics live outside the chart. In most general EHRs, an echo report is a PDF attachment. The ejection fraction inside it isn’t a data point the system understands — it’s a picture of a number. That means no automatic trending, no flags when a value crosses a threshold, and a lot of clicking back through documents to answer a simple question: what was her EF a year ago?
2. Documentation is built for billing, not cardiology. Generic templates force cardiovascular findings into one-size-fits-all note structures. Physicians either over-document to satisfy the template or dictate free text that locks the clinical detail away from any downstream use — quality reporting, research, registries.
3. Workflow assumes a generalist visit. A cardiology encounter often spans an office visit, a same-day echo, and a follow-up plan that depends on the result. General EHRs treat these as disconnected events in separate modules, with the physician serving as the human interface between them.
4. Quality and research are afterthoughts. Registry submissions, MIPS measures, and clinical trial screening all require structured cardiovascular data. When that data was never captured as data in the first place, practices end up paying staff to re-abstract charts manually.
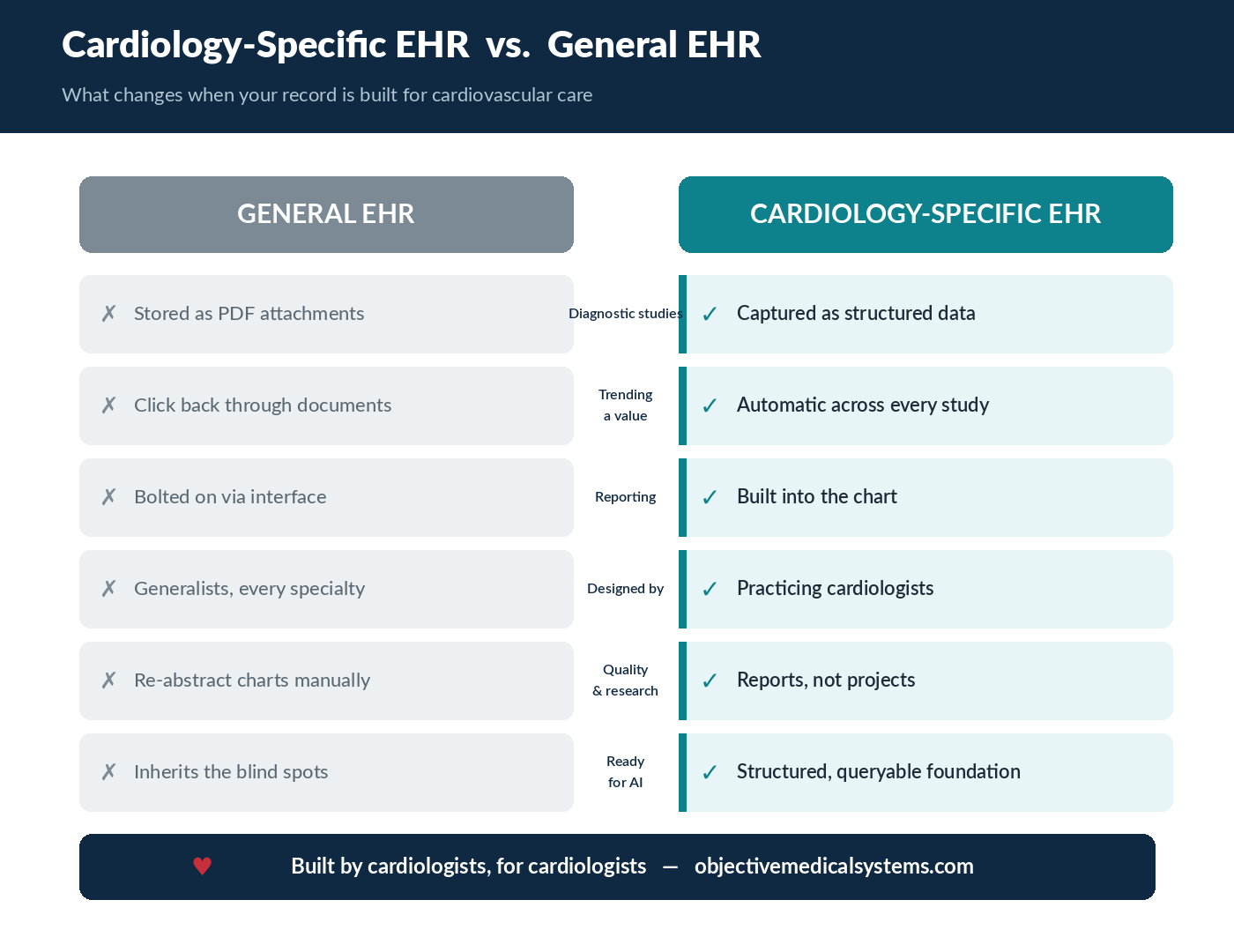
What “cardiology-specific” actually means
The term gets used loosely, so it’s worth being concrete. A cardiology-specific EHR is not a general EHR with a cardiology template pack. The difference shows up in the architecture.
Structured cardiovascular data from the start. Every study — echo, cath, nuclear, vascular — is captured as discrete, structured data, not a scanned report. At OMS, that adds up to more than 6,000 data points per patient, which is what makes trending, decision support, and analytics possible at the point of care.
Integrated diagnostic reporting. When structured reporting is part of the same system as the chart, the cardiologist reads a study, finalizes a report, and populates the record in one motion. No interface lag, no transcription step, no PDF graveyard.
Workflows designed by people who run clinics. OMS was built by practicing cardiologists who were frustrated by the same screens you are. That heritage shows in small things — how a normal echo can be reported in seconds — and big things, like how the system surfaces the prior data that actually changes today’s decision.
A platform that newer AI tools can stand on. Ambient documentation and AI assistants are quickly becoming standard expectations, but an AI layer is only as good as the data underneath it. Tools like AskOMS can answer questions about a patient’s cardiovascular history precisely because that history exists as structured data rather than stacked PDFs.
Why this matters more in 2026
The gap between general and specialty EHRs is widening, not narrowing, because of AI. Industry analysts expect the large majority of EHR interactions to involve some level of AI assistance by late 2026, and early research at major academic health systems has found measurable reductions in clinician burnout among physicians using ambient documentation tools.
But here’s the catch every cardiology practice should understand: ambient AI built on a general EHR inherits that EHR’s blind spots. An AI scribe can draft a beautiful note, but it can’t trend an ejection fraction that was never captured as data. The practices that will get the most out of this wave of AI are the ones whose underlying records are structured, cardiovascular-specific, and queryable — which is an architecture decision, not a feature toggle.
The business case, not just the clinical one
Specialty fit isn’t only about physician sanity. It compounds across the practice:
- Throughput. When documentation and reporting stop consuming evenings, capacity opens up. In OMS’s partnership announcement with MedAxiom, practices using the platform reported patient volume and throughput increases of 20–30%.
- Revenue integrity. Structured findings support more complete coding. Missed diagnoses are missed reimbursement — and missed risk-adjustment.
- Quality programs without abstraction labor. When the data is structured, MIPS measures and registry submissions become reports, not projects.
- Compliance confidence. OMS’s platform is ONC-certified, including HTI-1 certification for advanced decision support and predictive models — a bar many specialty vendors haven’t cleared.
“But switching EHRs is painful”
It is — and pretending otherwise is how vendors lose trust. Any practice that has lived through a conversion knows the real costs: data migration, retraining, a temporary productivity dip, and the political work of getting every physician on board. Three things make the calculation different than it was a decade ago.
The status quo has a price too. Practices tend to measure switching costs precisely and status-quo costs not at all. An hour of after-hours documentation per physician per day, multiplied across a group and a year, is an enormous number that never appears on any invoice. So is the revenue from studies that were performed but never fully coded.
Migration is a known problem now. Specialty vendors have done hundreds of conversions from the major general EHRs. The path from your current system — including historical diagnostic data — is well-worn, and a credible vendor will walk you through exactly what transfers as structured data versus what arrives as documents.
Interoperability standards have matured. With FHIR-based exchange now mandated and certified, a specialty EHR no longer means an island. OMS publishes its FHIR endpoints and maintains ONC certification precisely so cardiology practices can stay connected to hospitals, HIEs, and referring physicians while running a system built for their specialty.
The honest framing isn’t “switching is easy.” It’s that the pain of switching is paid once, while the pain of a poor-fit EHR is paid every clinic day, indefinitely.
Questions to ask any EHR vendor
If you’re evaluating systems, five questions separate true cardiology platforms from re-skinned general ones:
- Is an echo report stored as structured data or as a document?
- Can I trend any cardiovascular value across every study type without opening files?
- Was the reporting module built into the EHR, or bolted on through an interface?
- Who designed the clinical workflows — engineers, or practicing cardiologists?
- What certifications back the decision-support and predictive features?
The bottom line
A general EHR asks cardiologists to adapt to the software. A cardiology-specific EHR adapts to how cardiovascular care actually works — and in a specialty drowning in data and short on time, that difference shows up in throughput, revenue, quality scores, and how early you get home.
See the difference in your own workflow. Book a demo with the OMS team.
